


Summary:
It is a weak assumption that if employed physicians just stay busy, the financial model will be productive.
It is a weak assumption that if employed physicians just stay busy, the financial model will be productive. Indeed, there is a definable science to the success of the enterprise strategy within the IHS.
As health systems adopt a strategy of integration, they often proceed under the assumption that if the physicians and other providers employed just stay busy, the financial model will be productive.
PHYSICIAN LEADER COACH SERIES
This six-part series by Daniel K. Zismer, PhD, introduces an important competency and prepares physician leaders to function at the intersection of health strategy and enterprise risk. It was originally published by AAPL in 2016.
Part 1: Managing the Productivity of Enterprise and Risk Strategy
Part 2: Accountability for Health Care Leaders as Officers
Part 3: Clinically Integrated Network Strategy and the Role of Physician Leaders
Part 4: Operating Economics of Employed Providers in Integrated Health Systems
Part 5: Due Diligence and Integration
Part 6: Brand Campaigns, Brand Promises, and Enterprise Risk
An unappreciated vulnerability of the assumption lies with a sufficient understanding of the definition of productivity as it relates to the provider enterprise within integrated health systems, or IHS.
A lesson, frequently learned the hard way, is that you can’t aggregate providers under a loosely structured operating model, multiple compensation plans and cultures, turn them loose to their own devices and expect a business model to be productive at levels required of a health system’s strategic and business plan.
Principles provided here will help guide physician leaders as they field questions such as:
Why do we lose money on employed doctors?
Is our provider compensation plan working?
Why do our physicians refer outside of our system?
The Architecture of the Accounting
Before physician leaders attempt to fix the financial performance of the physician/provider enterprise within the IHS, they are advised to understand the accounting practices applied.
Call it the architecture of the accounting.
What does this mean? In the simplest of terms, the architecture of the accounting tells the story of how revenues, operating expenses and net operating margins of the enterprise are accounted within the IHS. The architecture of the accounting is influenced by the design and structure of the physician/provider enterprise, accounting procedures applied and the management philosophy of IHS leadership. Let’s breakdown the relevant concepts to their fundamental forms. We’ll start with structure.
It is often the case that physicians and other licensed providers are employed by a controlled corporate subsidiary or division within an IHS. (See Figure A .)
The anatomy of the financial structure of this corporate subsidiary or identified controlled division typically includes:
Professional fees generated by licensed providers.
Direct operating expenses accounted to the structure, including all provider and staff compensation and benefits, supplies, facilities used, direct expenses allocated for billing, collections, patient services accounting, marketing, professional liability insurance and other direct operating expenses identified.
Allocation of indirect, IHS overhead expense (including costs of capital).
Also, perhaps, some office-based ancillary services revenues.
Generally accepted accounting principles observations:
Operating revenues for the provider enterprise will often be restricted to professional fees. Most outpatient ancillary services and inpatient revenues will be billed from licensed facilities within the IHS.
Operating expense allocations for physicians/provider enterprise will include all direct operating expenses of sites, indirect operating allocations (services required to operate the provider enterprise) and corporate overhead allocations.
Net operating margin of the physician/provider enterprise will be negative, creating accumulating net operating losses within the controlled physician/provider enterprise within the IHS.
Most outpatient ancillary services revenues and patient services revenues generated for inpatient care are accounted to the entity within the IHS where the services are housed (entities outside the accounting boundaries of the physician/provider enterprise). Most typically, these services are housed within licensed hospitals or licensed outpatient services entities controlled by the IHS.
The consequences of properly applied, general accepted accounting principles is a negative operating margin produced by the physician/provider enterprise. The technically correct, but misguided conclusion drawn by many senior leadership teams and IHS boards is that employed physicians lose money. So while finance officials within the IHS can properly report such a conclusion to senior teams and the board, the truth is all productive physician/provider enterprises lose money given the nature of the architecture of the accounting. In fact, no (or few) larger independent multispecialty or single specialty medical group practices will operate from a model that delivers professional fees only; they all own profitable ancillary services, possibly including diagnostic services, ambulatory procedures and, sometimes, specialty hospitals.
What is important is not accounted losses; it is the economic and financial productivity of the physician/provider enterprise within the IHS; the ability of the organized entity to be economically and financially productive within the strategic plan and business model led and managed by IHS physician leadership.
What Affects Economic Productivity
The factors that most directly affect the economic productivity of the controlled physician/provider enterprise are:
The size, scale and clinical specialty mix of the employed physician/provider group. If, for example, the IHS employs primary care providers only — leaving the specialties to independent practitioners who own their own ancillary services — the economics of the physician/provider enterprise, and the IHS overall, will be especially challenged.
The compensation model and its relationship to provider productivity expectations is important. The issue is alignment of incentives; the alignment of physician compensation incentives with the productivity requirements of the provider enterprise strategy within the IHS. The failed assumption is if physicians stay busy the economics will work. Physicians can stay busy creating operating economics that are more or less productive for the IHS.
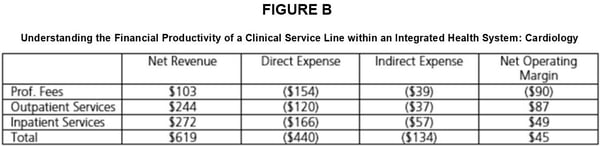
Physician leaders need to understand the connections between physician productivity profiles and the downstream economic productivity of the integrated model. (See Figure B.)
The extent to which the clinical model and provider referral behaviors capture the referral potential of the model. Referral leakage is a principal vulnerability of many integrated health systems in their early stages of development. Although there are legitimate reasons patient referrals leave the IHS (availability, access and patient preference), the viability of the integrated model is directly related to its ability to retain the clinical care demand it is designed to provide.
{kind=link}
Observations:
All estimates are provided on a per work relative value unit (wRVU) basis calculated based upon a 20-physician, subspecialized cardiology practice embedded in an IHS structure.
Professional fees generated create a net operating loss per wRVU provided.
All other clinical services generated throughout the service line are profitable to varying levels.
Net annual operating revenue for the model presented is $123,800,000 (20 FTE cardiologists producing, in the aggregate, 200,000 wRVUs annually).
Net margin per wRVU produced is $45; or an estimated $9,000,000.
(Note: Sample data provided by CliftonLarsonAllen .)
Conclusion
Form does follow function when contemplating design strategy and productivity of the provider enterprise within an IHS. It is a fool’s errand to hire physicians and other clinical providers as employees of an IHS, provide them no structure, leadership, sense of mission, vision, values or strategic direction, tell them to “just see patients” and expect the model to produce financially and economically at levels sufficient for success.
There is a definable art and science to the success of the provider enterprise strategy within the IHS. Physician leaders often stand alone in the IHS C-suite as the individual expected to know how it all should work. After all, you’re one of them.
This lesson merely scratches the surface of the big issue: leading the strategic productivity of what is arguably the most important economic flywheel of the IHS, the provider enterprise.

Daniel K. Zismer, Ph.D, is a founder and managing director of Castling Partners, a consultancy focused on strategy performance and integrative risk management for health and health care organizations. Zismer has a 30-year career in the leadership of health care organizations and executive education. His area of specialization is strategy and the performance of strategy. He is the Wegmiller Professor Emeritus, School of Public Health, University of Minnesota Programs in Health Care Administration.
Topics
Strategic Perspective
Accountability
Motivate Others
Related
The Right Way to Process FeedbackFast Thinkers Are More Charismatic“Profiles in Success”: Certified Physician Executives Share the Value and ROI of their CPE EducationRecommended Reading
Motivations and Thinking Style
The Right Way to Process Feedback
Motivations and Thinking Style
Fast Thinkers Are More Charismatic
Professional Capabilities
“Profiles in Success”: Certified Physician Executives Share the Value and ROI of their CPE Education
Professional Capabilities
From the Idea to the Business Plan: Evaluating the Opportunity
Problem Solving
Effective Patient Scheduling
Problem Solving
Project Managers, Focus on Outcomes — Not Deliverables